
Does raising drug prices reduce opioid deaths?
An application of price theory from Casey Mulligan

Imagine you’re a policymaker trying to tackle the opioid crisis. You decide to crack down on prescription opioids, making them harder to get. Surely this will reduce opioid use and save lives, right? After all, raising prices reduces the quantity demanded.
Well, not so fast. Researchers have found that, at other times, tighter prescription regulations actually led to more opioid deaths. So do higher prescription costs save or cost lives?
This question is at the heart of Casey Mulligan’s forthcoming JPE paper, “Prices and Policies in Opioid Markets.” Mulligan doesn’t just document these seemingly contradictory trends; he provides a compelling explanation using the tools of price theory. Mulligan combines a simple model with careful empirical work to shed light on a vital real-world issue.
Mulligan’s key insight is that the effect of prescription policies depends crucially on the “price gap”—it’s always about relative prices—between prescription (Rx) and illicitly manufactured (Im) opioids. When prescription prices are much higher than Im prices, tightening prescription regulations can push people to cheaper illicit sources, potentially increasing overall consumption and mortality. But when prescription prices are lower, increasing prescription supply can act as a "gateway" to opioid use, also increasing mortality.
As much as the topic of opioids is of first-order importance, what I love about this paper is how it showcases the power of empirical price theory. Mulligan starts with a simple model of consumer choice between prescription and illicit opioids. By thinking carefully about the incentives and trade-offs involved, he generates surprising insights that help make sense of the data. This approach - using basic economic logic to understand complex phenomena - is price theory at its best. It’s not about elaborate models or fancy econometrics (though those have their place). It’s also not just about blog posts. It’s about really thinking through how people respond to incentives and how markets work, whether that’s in every day commentary or in academic research.
So today, we’re going to walk through Mulligan’s analysis as an example of price theory as research tool. We’ll see how he models the opioid market, what predictions his model makes, and how he tests those predictions empirically. Along the way, we’ll learn some valuable lessons about how to apply price theory to thorny real-world problems.
A Simple Model of Legal and Illegal Drug Sources
At the heart of Mulligan’s analysis is a key insight: consumers of opioids face a nonconvex budget set. What does this mean? Essentially, consumers have access to two sources of opioids - prescription (Rx) and illicitly manufactured (Im). Each source has its own fixed costs (think of the hassle of getting a prescription or finding a dealer) and marginal prices per unit.
Here’s the crucial bit: Mulligan shows that this setup can lead to a situation where consumers face a high marginal price at low levels of opioid consumption and a low price at high levels. This nonconvexity in the budget set can cause some surprising outcomes and differs from the normal reasoning, where higher demand pushes up prices. We need to look at the supply side too, and with fixed costs, the supply curve can slope down. Elsewhere, Mulligan has called this personalized increasing returns.

For instance, as prescription prices rise, some consumers might suddenly find it optimal to switch from prescription to illicitly manufactured sources. This switch doesn’t just change their source—it can lead to a discrete jump in their total consumption. While illicitly manufactured might have higher fixed costs, its marginal price could be much lower.
This insight drives much of Mulligan’s analysis and leads to some counterintuitive predictions. It suggests, for example, that tighter prescription regulations could sometimes increase overall opioid consumption by pushing people to cheaper illicit sources.
Let’s dive deeper into Mulligan’s model, its predictions, and how he tests them empirically. Along the way, we’ll see how this work exemplifies the power of the price theory approach in tackling complex real-world issues.

Take a look at Figure 1b from the paper. Point B represents consuming only prescription opioids. This is the initial optimal bundle for a consumer. The crucial insight is that a small increase in prescription prices can cause a consumer to jump from B to C, discretely increasing their total opioid consumption. Point C represents consuming illicitly manufactured opioids (or a mix of prescription and Im). This kind of discontinuous behavior is key to understanding the market dynamics.
From this setup, Mulligan derives several important results. As prescription prices rise, some consumers switch to illicitly manufactured sources. This can lead to higher total consumption if illicitly manufactured prices are low enough. The effect of prescription prices on total consumption depends critically on the gap between prescription and illicitly manufactured prices. When illicitly manufactured prices are much lower, tighter prescription regulations can increase overall consumption.
The Gateway Hypothesis
One of the most intriguing aspects of Mulligan’s model is how it provides a simple way to capture the “gateway hypothesis” in opioid markets. This isn’t just about short-term substitution between sources—it’s about how policies today can shape consumption patterns far into the future. This comes out of the rational addiction, or habit formation, literature.
Here’s the key idea: Mulligan models consumers as starting their “opioid career” with low levels of consumption and typically using prescription opioids first. Why? Because prescription opioids usually have lower fixed costs of access - it’s easier to get a prescription than to find an illicit dealer, especially for young people. But as people consume more opioids over time, their “taste” for opioids (represented by a parameter θ in the model) increases. This captures the idea of growing tolerance or addiction. Eventually, some consumers find it worthwhile to switch to illicit opioids, which might have higher fixed costs but lower marginal prices.
This process creates a “gateway” from prescription to illicit opioids for some consumers. Importantly, it suggests that policies affecting prescription access today could have long-lasting effects on future illicit opioid use.
Mulligan formalizes this idea through a long-run demand function that captures how past consumption affects current demand. This allows him to analyze both short-run and long-run policy effects, which can sometimes go in opposite directions. For example, tightening prescription regulations might increase overall opioid consumption in the short run by pushing current users to cheaper illicit sources. But in the long run, it could reduce consumption by preventing new users from starting on the “gateway” path.
This framework helps explain some of the puzzling empirical patterns we see in the data, like different policy effects for different age groups or changing racial disparities in opioid use over time. It’s a great example of how careful economic modeling can provide new insights into complex social problems.
Empirical Tests and Findings
So we have a simple model of consumer choice, combined with some reasoning about what affects the taste for opioids parameter. Now, Mulligan doesn’t just leave us with theory. He puts his model to the test using data on opioid deaths and a comprehensive database of federal opioid policies he constructs.
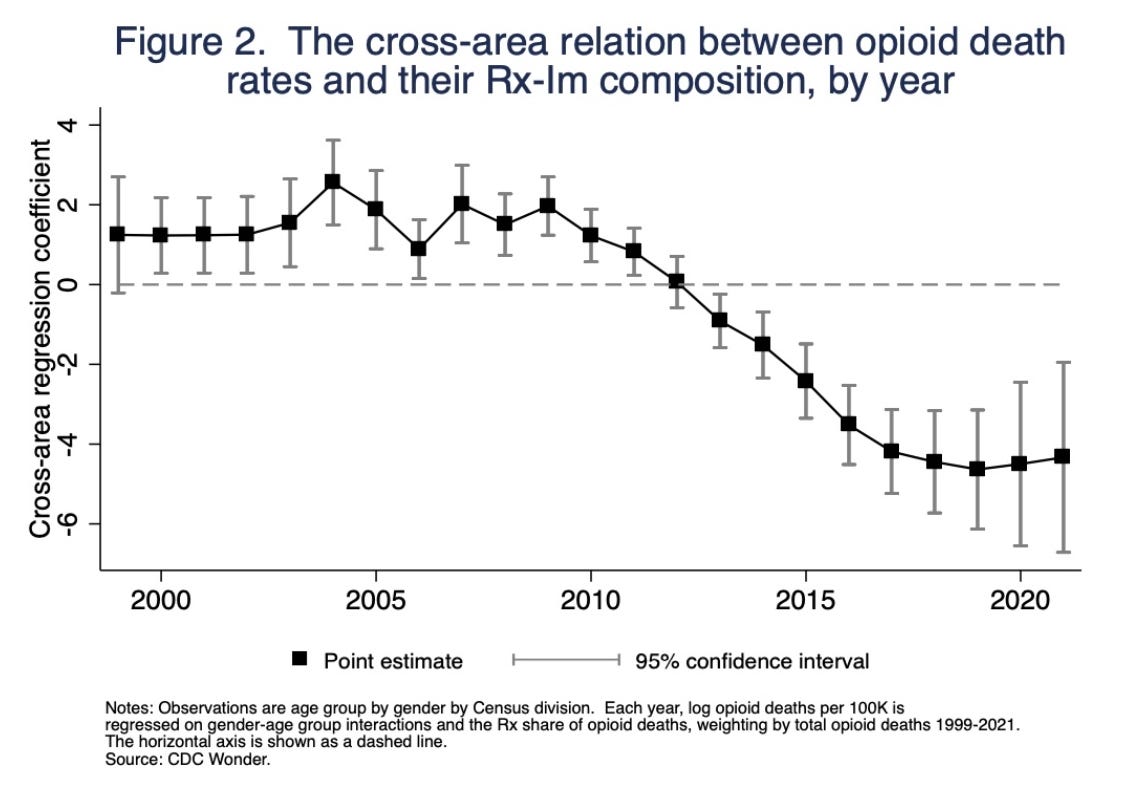
For instance, Mulligan's model suggests that when the cost of illicit opioids decreases, people might switch from prescription opioids to these cheaper alternatives. This shift would reverse the previously observed trend where higher prescription rates correlated with higher death rates. Around 2012-2013, this is exactly what happened: the correlation between opioid death rates and prescription shares flipped as illicit opioid prices fell, showing how users might have transitioned to cheaper illicit options.
A second test is whether the 2010 OxyContin reformulation and new regulations affected opioid deaths. Previous studies found mortality roughly constant. How is that possible? Remember, there are two effects: One is pushing people toward more dangerous illicit drugs, and the other is stopping people from starting using at all. Mulligan shows how fatalities fell for children and youth, whose opioid consumption appeared to be especially prescription intensive while rising for adults. Combined you get the zero effect for the overall population.

The Power of Price Theory
Again, I think this paper is worth studying as an example of how to do price theory in practice. I’m often asked what price theory is and what makes it unique. It’s worth first pointing out that it involves theory. That’s not a given in research on opioids, even within economics. A lot of papers in this area focus on reduced-form empirics. They look for natural experiments in opioid policy and measure impacts on outcomes. That’s valuable work, but it often lacks a unified framework for interpreting results across studies. Why would deaths sometimes rise and sometimes fall? While other papers might discuss elasticities, they don't specify which elasticities matter for explaining why opioid mortality might increase with prescription prices.
Beyond that, the type of theory is unique. In the paper, Mulligan points out a crucial gap in existing research. He notes that “Medical experts advising or serving as policymakers typically ignore the interplay between (prescription) and (illicitly manufactured) delivery channels.” Even major policy recommendations often fail to consider how changes in prescription regulations might affect illicit markets.
Mulligan argues that his economic model "suggests a different approach." By explicitly modeling consumer choice between prescription and illicit opioids, he captures crucial interactions that other analyses miss. This isn't just an academic exercise - it has real policy implications. For instance, it shows how tightening prescription regulations could potentially increase overall opioid consumption by pushing people toward cheaper illicit sources.
Remember our answer to the question, what is price theory?

First, price theory is fundamentally about exchange. Opioids are purchased in markets, legal or illegal. It’s all about how consumers choose between different sources of opioids.
Second, prices are crucial to how things play out in those market. The relative prices of prescription and illicitly manufactured opioids determine not just quantities consumed but also which source consumers use.
Third, Mulligan uses a simple but powerful model. The core insights come from a straightforward consumer optimization problem. Yet this simple setup yields non-obvious predictions.
I’ve already argued that Mulligan's approach offers several advantages over these alternatives. It provides a consistent framework for interpreting seemingly contradictory empirical findings. It generates non-obvious, testable predictions. And it clarifies key economic forces in a way that aids policy analysis. Perhaps most importantly, it avoids common pitfalls like assuming away the illegal market or reasoning from a price change without considering causes. By modeling both prescription and illicit markets together, Mulligan captures crucial dynamics that other approaches miss.
This research shows the enduring value of price theory for understanding complex real-world phenomena. It's not just about supply and demand curves. It's about using core economic principle—optimization, prices as signals, substitution effects0to shed light on vital issues.
So, next time someone asks you, "What is price theory good for?," you can point them to opioid markets. Careful thinking about prices and exchange can really help inform policies that save lives.
What a fantastic read!
It's also really important to understand the mechanism by which opiods cause harm and death. Many people naturally assume that decreasing the consumption of unnecessary opiods is the superior policy outcome but that is often going to be wrong.
After all, the best ways we have to treat opiate addiction are by giving the patient large but stable doses of opiates. When possible this is now via partial mu-agonists like buprenorphine which have the benefit of both a ceiling effect and of blocking the effect of other opiates but the older (and still appropriate for those with pain or very high tolerances) treatment was just administering methadone -- basically just a cheap long lasting strong opiate.
These treatments are effective because the actual harm caused by opiate addiction is largely as a result of people going through cycles of withdrawal and intoxication -- especially when that cycle results in a drop in tolerance and an overdose. In itself the intoxication isn't harmful but it can certainly lead to bad deciscions.
This suggests that optimal opiate policy may not actually always want to reduce overall unnecessary consumption -- treatment may be better but absent that it's still better for addicets to have steady rather than intermittent access.
Indeed, it actually raises the question if it wouldn't be superior for the government to flood the illicit market with cheap (generally somewhat less euphoric) long acting partial agonists like buprenorphine.